



Home / Training / Manuals / Atlas of breast cancer early detection / Cases
Atlas of breast cancer early detection
Go back to the list of case studies
.png) Click on the pictures to magnify and display the legends
Click on the pictures to magnify and display the legends
| Case number: | 052 |
| Age: | 67 |
| Clinical presentation: | Postmenopausal woman with average risk of developing breast cancer presented with a lump in the left breast. Examination revealed a hard 2 cm lump in the upper inner quadrant of the left breast. |
Mammography:
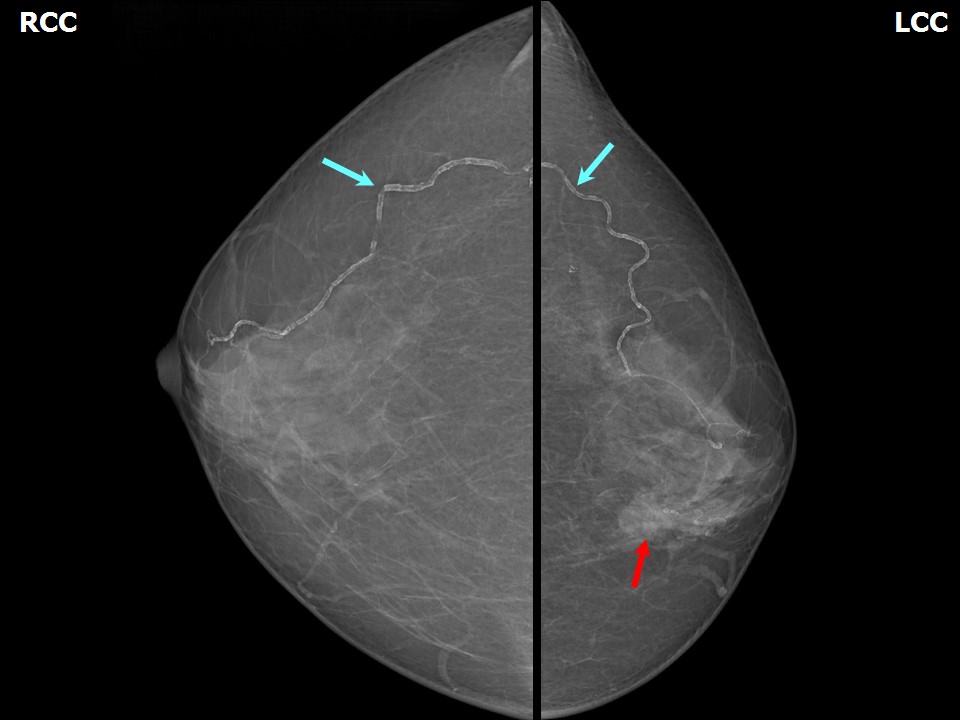 | 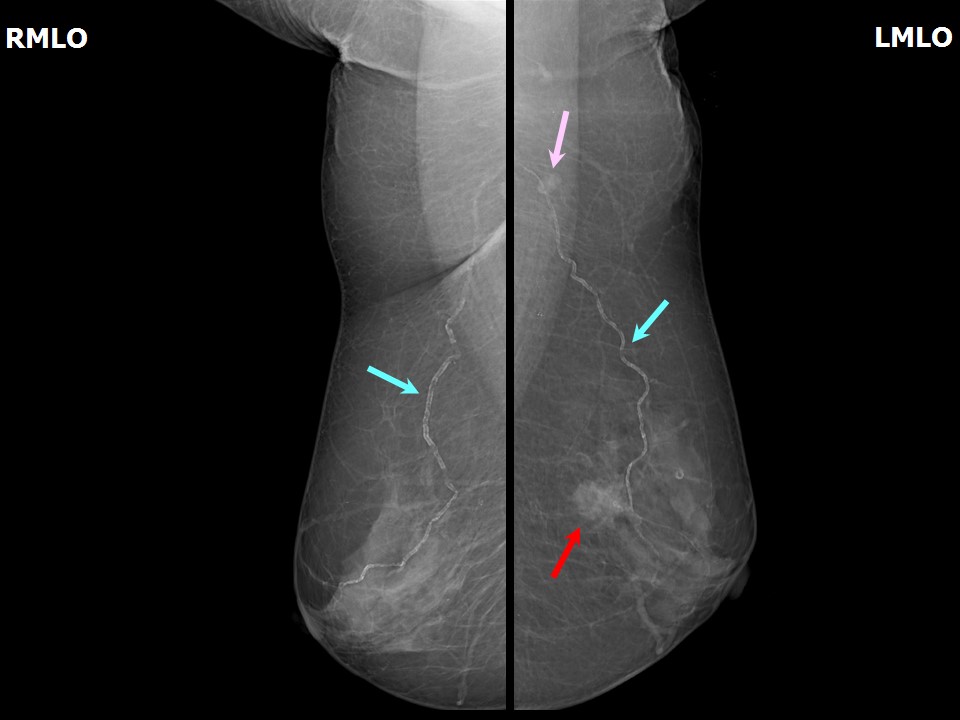 |
| Breast composition: | ACR category b (there are scattered areas of fibroglandular density) | Mammography features: |
| ‣ Location of the lesion: | Left breast, upper inner quadrant at 11 oclock, middle third |
| ‣ Mass: | |
| • Number: | 1 |
| • Size: | 2.0 × 1.0 cm |
| • Shape: | Irregular |
| • Margins: | Indistinct |
| • Density: | Equal |
| ‣ Calcifications: | |
| • Typically benign: | Vascular calcification |
| • Suspicious: | None |
| • Distribution: | None |
| ‣ Architectural distortion: | None |
| ‣ Asymmetry: | None |
| ‣ Intramammary node: | None |
| ‣ Skin lesion: | None |
| ‣ Solitary dilated duct: | None |
| ‣ Associated features: | None |
Ultrasound:
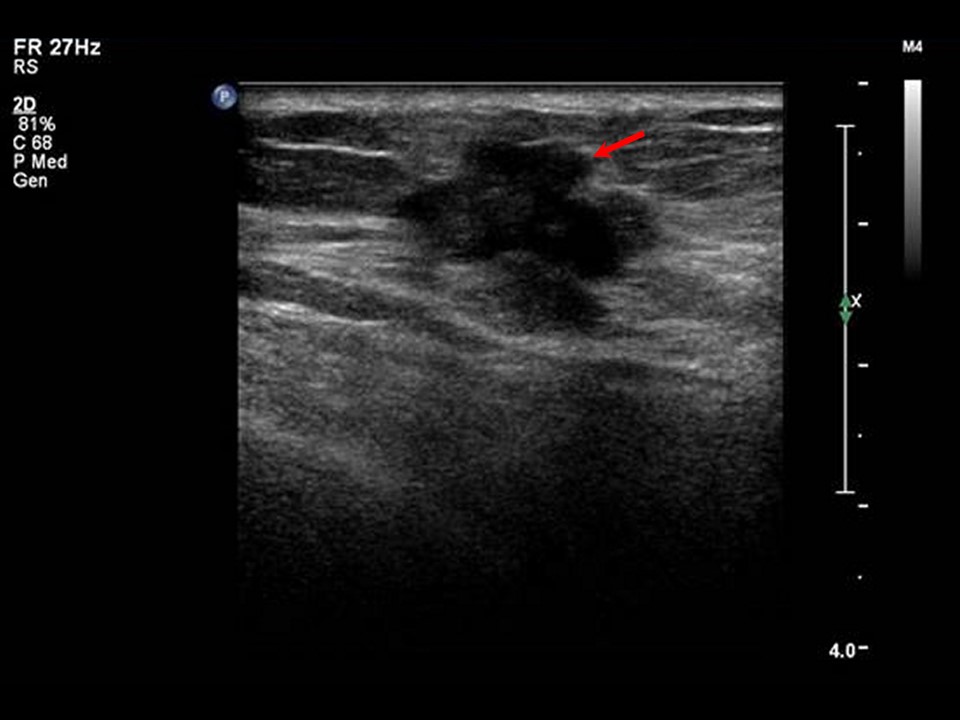 |  |
| Ultrasound features: Left breast, upper inner quadrant at 11 oclock position | |
| ‣ Mass | |
| • Location: | Left breast, upper inner quadrant at 11 oclock position |
| • Number: | 1 |
| • Size: | 1.9 x 1.5cm |
| • Shape: | Irregular |
| • Orientation: | Not parallel |
| • Margins: | Angular |
| • Echo pattern: | Hypoechoic |
| • Posterior features: | No posterior features |
| ‣ Calcifications: | None |
| ‣ Associated features: | Internal vascularity |
| ‣ Special cases: | None |
BI-RADS:
BI-RADS Category: 5 (highly suggestive of malignancy)Further assessment:
Further assessment advised: Referral for cytologyCytology:
 |
| Cytology features: | |
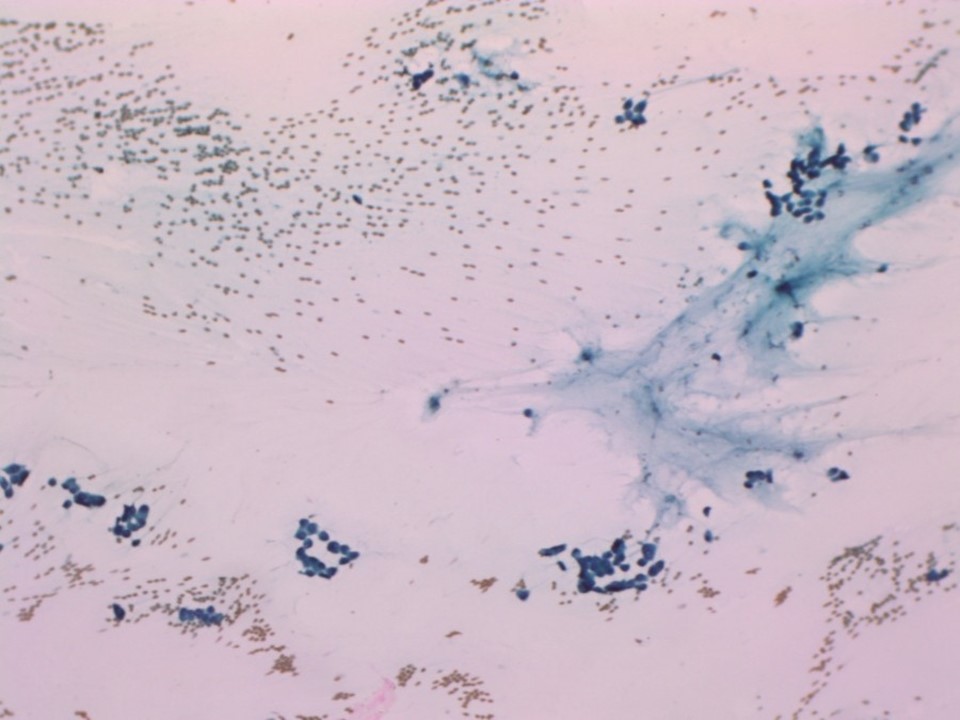
| ‣ Type of sample: | FNAC |
| ‣ Site of biopsy: | |
| • Laterality: | Left |
| • Quadrant: | Upper inner |
| • Localization technique: | Palpation |
| • Nature of aspirate: | 0.2 mL of mucoid material |
| ‣ Cytological description: | Smears reveal many loosely cohesive clusters and sheets of malignant cells. Many cells show a plasmacytoid appearance. There are a few fibroadipose tissue fragments and mucinous material in the background |
| ‣ Reporting category: | Malignant |
| ‣ Diagnosis: | Carcinoma low grade |
| ‣ Comments: | None |
Histopathology:
Lumpectomy
 |
| Histopathology features: | |
| ‣ Specimen type: | Lumpectomy |
| ‣ Laterality: | Left |
| ‣ Macroscopy: | Specimen (7.5 × 5.5 × 5.0 cm) with skin flap (6.0 × 3.6 cm). On serial sectioning, a firm greyish white area (1.8 × 1.2 × 0.8 cm) with gelatinous appearance is identified. An area of fibrosis (3.5 × 2.5 cm) is seen towards the lateral side. The tumour is located 0.7 cm from the skin (anterior margin), 1.5 cm from the posterior margin, 2.0 cm from the superior margin, 1.0 cm from the inferior margin, 1.8 cm from the medial margin, and 3.5 cm from the lateral margin |
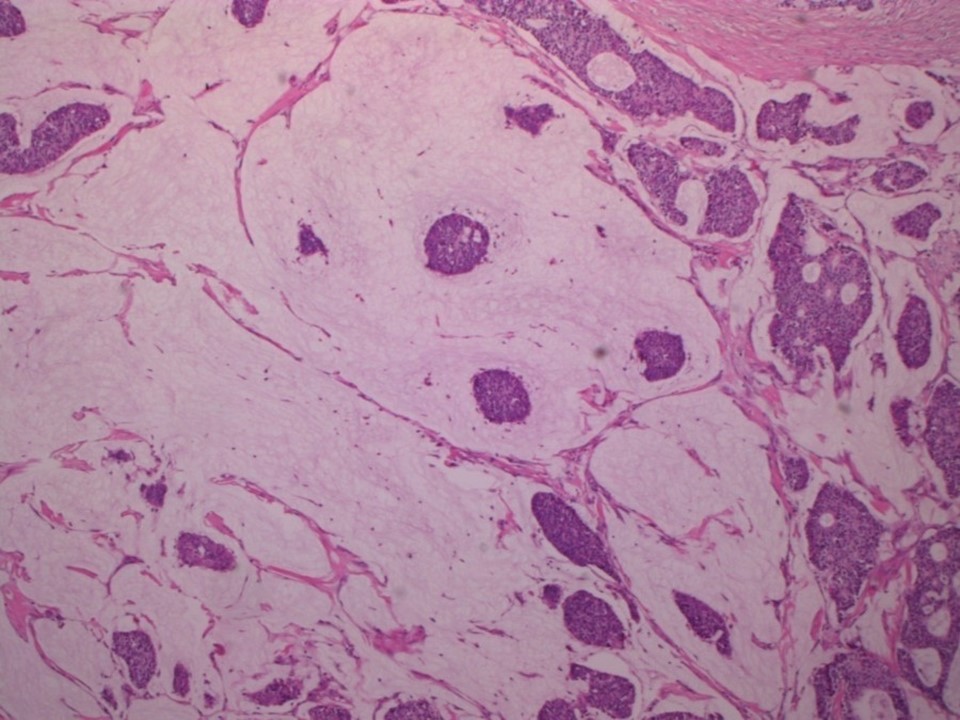
| ‣ Histological type: | Mucinous carcinoma with neuroendocrine differentiation. Tumour cells are arranged in a cribriform pattern and as solid nests in pools of extracellular mucin |
| ‣ Histological grade: | Grade 2 (3 + 2 + 1 = 6) |
| ‣ Mitosis: | 3 |
| ‣ Maximum invasive tumour size: | 1.8 cm in greatest dimension |
| ‣ Lymph node status: | 0/26 |
| ‣ Peritumoural lymphovascular invasion: | Present |
| ‣ DCIS/EIC: | Absent |
| ‣ Margins: | Free of tumour |
| ‣ Pathological stage: | pT1N0 |
| ‣ Biomarkers: | |
| ‣ Comments: |
Case summary:
| Postmenopausal woman presented with left breast lump. Diagnosed as left breast carcinoma, BI-RADS 5 on imaging, as mucinous breast carcinoma on cytology and as mucinous carcinoma with neuroendocrine differentiation, pT1N0 on histopathology. |
Learning points:
|